
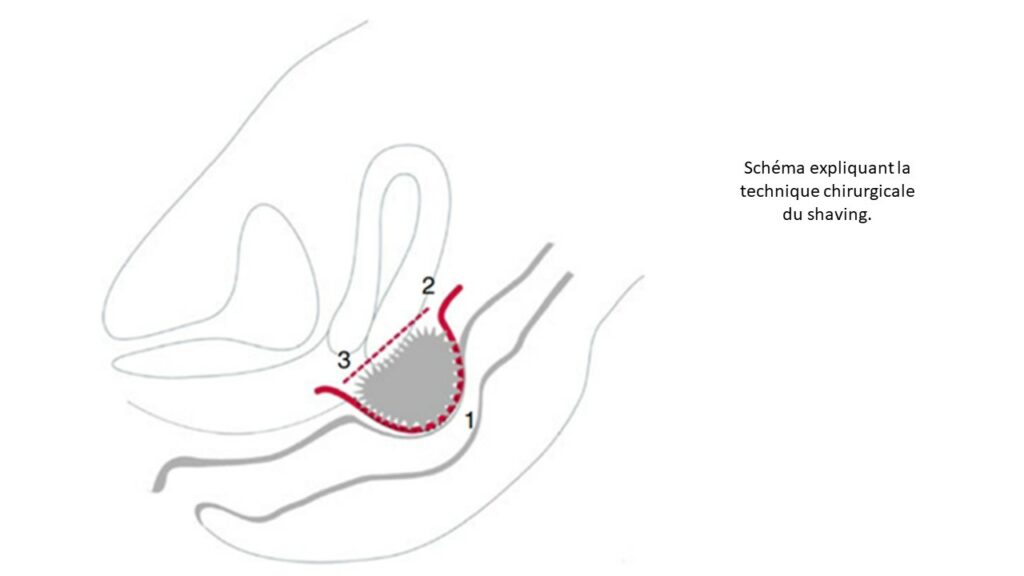
Shaving, often wrongly considered to be a superficial treatment, involves complete excision of rectal endometriosis while preserving its integrity (12, 13, 15, 19). This is a delicate procedure requiring specific training in which the CEC has particularly extensive experience. Indeed, in a study of more than 3,190 patients operated on using the CO2 laser shaving technique, more than 90% saw their quality of life improve and 84% of patients suffering from infertility were able to subsequently conceive 57% of them spontaneously (12, 17, 19).
This surgical technique is also associated with a very low rate of complications. One of the most dreaded complications like rectovaginal fistula (requiring a temporary stoma) is encountered in 0.06% in our experience (13, 15, 17). This low rate remained constant even in a series of more than 700 patients whose lesion size exceeded 4 cm. In our practice, a stoma is never placed as a preventive measure, but only in the event of postoperative complications such as digestive fistula., By preserving the neurological plexuses, shaving allowed all the patients in our series to be able to empty their bladder without having to resort to intermittent catheterization(13, 15, 17).
The risk of recurrence is also low, just 3.6% after pregnancy (12). The only randomized study comparing various operative techniques shows a similar recurrence rate between the different techniques (shaving, discoid resection and rectal resection)(20).
We therefore consider shaving to be the technique of choice, as it can successfully surgically treat over 95% of deep rectal endometriotic lesions (15, 19). It is important to point out that any decision to preserve the rectum must be taken preoperatively and validated in a multidisciplinary meeting.
However, rectal shaving is not feasible in three specific situation(15): n case of major stenosis with posterior rectal invasion (more than 90% of the rectal lumen), when the endometriotic lesion extends beyond the digestive mucosa (confirmed by colonoscopy with biopsy), in the event of sigmoid endometriosis. These circumstances, arising in 5% of patients in our experience, require recourse to other techniques, such as discoid resection or rectal resection
(19).
Lesion size is not an argument for choosing one technique over another and the 3 cm threshold justifying radical surgery should be discarded. This rule is not part of our decision tree.